
(This article was published originally 3 years ago, some of the content has been changed from it’s previous publication)
If we learned anything from Week 16 and the Wild Card round of the playoffs, it’s that watching someone tear their ACL remains one of the most gruesome things to experience, whether it’s in person or while watching TV. Sitting at a friend’s house watching the 49ers/Seahawks game during Week 16, I knew it the second I saw it that Mario Manningham tore his ACL. I actually remember saying that I thought he tore both his ACL and MCL, mainly based on how much his knee dove in when he got his foot caught underneath his body. Same goes with watching RGIII this past weekend against the Seahawks, although initial reports say that he only has partial tears of the ACL and MCL. Maybe short of a broken bone, nothing makes me cringe more than seeing an athlete tear his ACL, partly because it almost always seems like they KNOW they just tore their ACL and that the next year of their lives just changed in an instant. Despite the improvements in surgical intervention and rehabilitation, recovery post-ACL reconstruction remains both tricky to predict and a long, arduous process.
The point of this post today is not to point out what we already know: ACL tears are bad. But it’s to give you some insight into why exactly this small bundle of collagen fibers plays such a crucial role in an athlete’s function and what goes into the rehab process following this gruesome injury.
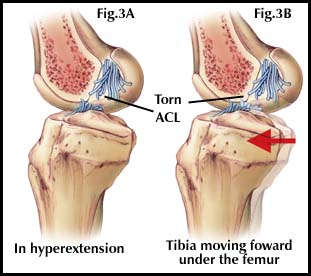
First question we have to answer: What is the ACL? Essentially, and very simply, the Anterior Cruciate Ligament (ACL) stops the tibia (shin bone) from gliding anteriorly (forward, towards the front of the body) on the femur (thigh bone). The significance of this knee ligament is that it provides the stability of the knee during movements such as planting-and-pushing-off, stopping quickly on a dime, cutting, and decelerating during a run/sprint. When you take this ligament away from a football player, it’s essentially taking away their burst, change of direction, and ability to accelerate/decelerate all in one pop (literally). Check out this diagram to get a visual of everything I just rambled on about:
Now that we understand the function of the ACL, our next question to answer is this: How does a person tear an ACL? Typically, the most common mechanism of injury (MOI) for an ACL tear is a twisting motion occurring at the knee while the foot is planted on the ground. This can happen with or without another player/person present, as it is quite common for an athlete to tear their ACL with no one anywhere near them (RGIII is a perfect example). What typically happens is the torsion that’s imparted on the knee places maximal strain on the ACL itself, and without the sufficient supporting joint and muscular strength to take on this force, the ACL overstretches. And with the right amount of excessive force, this leads to a partial or full tear of the ligament. Also, if the movement in question or the blow to the knee causes the knee to dive in enough, this is very commonly how people tear both the ACL and the Medial Collateral Ligament (MCL) and, potentially, medial meniscus at the same time. The MCL is the ligament that stops the knee from collapsing in when someone hits your knee from the outside. The combo platter of an ACL and MCL is typically a bit more tricky to surgically repair and rehab due to the addition of even more instability at the knee. Always remember, the more structures involved, the more difficult the rehab is.
Another common MOI with ACL tears is excessive knee hyperextension. When this happens, the femur can glide posteriorly (to the back) on a stable tibia when the foot is planted to the ground, which causes relative excessive anterior tibial motion. Think about what we said was the function of the ACL, stopping the tibia from moving anteriorly (forward) on the femur. Well, if you keep the tibia (shin bone) stable and move the femur posteriorly, it basically causes the same movement, except the femur is doing all the moving. This can also put strain on the Posterior Cruciate Ligament (PCL), which stops the tibia from moving posterior on the femur.
Ok, so we’ve gone over what the ACL is and how people tear their ACLs. Now, what goes into rehabbing this important ligament? Post surgery, the most important thing to regain is range of motion (ROM). Since a person is typically placed in a brace of some sorts (most of the time, depends on the doc) to help protect the new ligament, the knee becomes very stiff and does not move very well once the rehab process begins.
[Quick side note before we move on: When reconstructing the ACL, there are typically 3 options when deciding what type of graft to use: Your own patellar tendon, Your own hamstring tendon, or an ACL from a cadaver. Typically, cadaver grafts provide a good combination of quick recovery and great results long term, but there’s always the chance of rejection because you’re putting foreign tissue in your body and there’s increasing shift away from this now as more evidence becomes available. Patellar tendon grafts typically are super stable, but take a bit longer to heal because you’re using a tendon instead of a ligament, as tendons are not as pliable as ligaments. Also, taking a chunk of your patellar tendon can weaken your quadriceps muscle group significantly, as the patellar tendon attaches the quads to the tibia. Hamstring grafts are the last of the three options and allow the athlete to get back a bit faster than the patellar tendon choice and is arguably gaining more popularity now compared to 5-10 years ago]
While concurrently working on range of motion, initial strengthening of the quads, hamstrings, and gluts are in order, usually beginning with isometric strengthening (activating musculature without movement). In addition, it’s imperative to work on surgical scar mobility in order to allow the surrounding tissue to maintain its mobility and properly slide/glide on each other during motion.
The first phase of the rehab process is predicated on achieving 3 major milestones: 1- Regain proper quad muscle activation; 2-Decrease and minimize post-operative swelling; 3- Regain full range of motion, particularly full knee extension (straightening out the knee). Achievement of these three milestones is crucial before progressing to the next stage of rehab.
Following these initial phases in addition to the athlete being cleared by their orthopaedic surgeon, there’s a progression from isometric strengthening to isotonic, which involves moving resistance as muscle length changes. This progresses from mat exercises to sitting exercises to standing exercises, all based on achieving milestones before moving on to the next phase.
Once this phase is reached, we move on to dynamic movements, in straight lines first, then adding lateral and diagonal motions to help rebuild stability around the knee. This goes on until the individual is ready to do sport-specific exercises, which is the last step before return to play.
Last important question we need to answer is what is the prognosis for recovery from this terrible injury? This varies depending on the individual and whether multiple structures were involved, but as Adrian Peterson showed us, timetables can be thrown out the window when it comes to world class athletes. BUT, in general, prognosis for return to sport can be anywhere from 6 months to 12 months, depending on complications, past injury history, and response to rehabilitation. But as you’ve probably heard many times, a player in any sport is typically not back to their “prior level of function” until the second year following reconstruction.
This is by no means a set rule for all cases, but it takes time for an athlete to feel comfortable back on the field again, competing at the highest levels, without thinking about how to move and whether their knee with hold up to these enormous demands placed on it. One of the more difficult things for an elite athlete following this type of injury is getting back to moving instinctively, which is where a lot of the variability in return to sport comes from. Some get this back faster than others.
What does this mean for someone like Breshad Perriman. According to Ian Rappaport from NFL.com, he saw Dr. James Andrews today to determine the next step in his recovery process
#Ravens WR Breshad Perriman’s scope from James Andrews is tomorrow. That will determine if he needs a reconstruction. 1st visit was today.
— Ian Rapoport (@RapSheet) June 13, 2016
This is the tricky part of suffering a partial tear vs a full tear. With partial tears, due diligence needs to be performed in order to determine the severity and extent of the damage before jumping into making a decision on reconstruction vs conservative rehabilitation. The likelihood of Perriman going the conservative route, in my opinion, is slim. If he does, they’d take the rehab process on a week to week basis, determine his response to treatment, and ultimately see if he can get back on the field and perform at a high level while they give the ligament time to heal.
However, this road could still ultimately lead to reconstruction if conservative rehabilitation does not get the job done, which will end up costing him time on the back side. The one positive from attempting to rehab first would be that Perriman would be extremely strong and mobile going into the surgery, as PREhab has been shown to improve outcomes post-operatively. Regardless, and very unfortunately, I don’t think we’re seeing Perriman at all this year, which means we’re looking increased involvement of both Kamar Aiken and Mike Wallace this season barring a free agent signing.
Thanks for reading kids! Much more to come to help you get ready for the 2016-17 season.
